
by Mass General Brigham
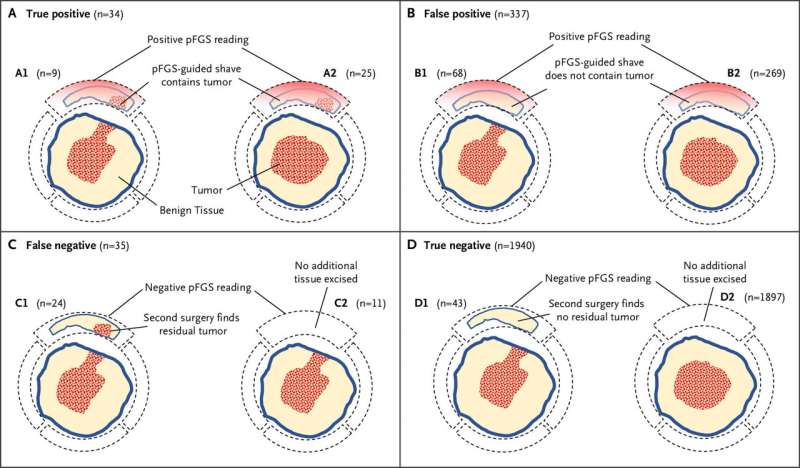
Margin Scoring Schema. Pegulicianine fluorescence-guided surgery (pFGS) readings (positive or negative) from each lumpectomy cavity orientation were compared with histopathology of the adjacent tissue to classify the pFGS signal as true positive (Panel A), false positive (Panel B), false negative (Panel C), or true negative (Panel D). Positive pFGS readings (Panels A and B) were compared with histopathology of the guided shave whether the prior margin in that orientation was positive (Panels A1 and B1) or not (Panels A2 and B2). Negative pFGS readings (Panels C and D) were compared with histopathology of tissue excised from the imaged orientation at a second surgery (Panels C1 and D1) or with the prior excised lumpectomy margin at that orientation if no additional tissue was excised (Panels C2 and D2). Credit: NEJM Evidence (2023). DOI: 10.1056/EVIDoa2200333
A new technique designed to allow surgeons to identify and remove residual tumor tissue during breast-conserving surgery showed promising results in a multi-center trial led by investigators from the Mass General Cancer Center, a member of Mass General Brigham. The clinical trial, which was funded in part by Lumicell, Inc., evaluated Lumicell's investigational optical imaging agent pegulicianine in fluorescence-guided surgery (pFGS).
In pFGS, pegulicianine is activated to a fluorescent form at sites of residual tumor, allowing surgeons to identify tumor remaining in the surgical site during breast cancer surgery. Investigators found that pFGS enabled removal of residual tumor cells left behind by standard lumpectomy procedures or avoided second surgeries in 10 percent of study patients. Results are published in NEJM Evidence.
"The goal of our research is to evaluate ways to improve the effectiveness of lumpectomy surgery, reduce the burden on patients and to help surgeons get to clean margins," said corresponding author Barbara Smith, MD, Ph.D., the director of the Breast Program at Mass General Cancer Center and head of the Breast Section in the Department of Surgery. "In our study, this intervention had a favorable effect for 10 percent of the patients that we studied. By evaluating margins in real time, surgeons can remove additional tissue immediately."
Traditionally, tumor margins are evaluated by pathologists after the tumor has been removed from the patient's cavity by surgeons. Tumor specimens are often deformed after they have been excised, making it challenging to evaluate margin orientation, and the return of results can take several days.
The pFGS approach involves injecting pegulicianine, a fluorescent dye, prior to surgery. After surgeons remove the initial tumor specimen, they use a hand-held probe to scan the lumpectomy cavity looking for additional tumor to remove. Image analysis software then displays any fluorescent signal on a screen, indicating remaining tumor tissue for removal.
To evaluate pFGS, Smith and colleagues conducted a prospective trial, enrolling 406 patients at 14 U.S. sites. All patients were undergoing lumpectomy for stages 1 to 3 invasive breast cancer and/or ductal in situ carcinoma (considered the earliest form of breast cancer). Among patients who were randomized to receive pFGS, surgeons performed their standard lumpectomy and then removed additional tissue based on pFGS guidance.
In 27 of 357 patients (7.6 percent) who underwent pFGS, the technique detected tumor tissue that had been left behind by standard lumpectomy. In the 17 percent of patients who had positive margins after standard surgery, 9 of 62 had all margins cleared by pFGS, potentially avoiding a second surgical procedure. pFGS had few safety events—the rate of allergic reactions was low and similar to that of other commonly used imaging agents.
The team also assessed diagnostic performance of pFGS by measuring the percentage of margins with tumor that were pFGS positive (sensitivity) and the percentage of margins with no tumor that were pFGS negative (specificity). Sensitivity was 49.3 percent across all study margins, and 58.6 percent for margins where direct histopathology comparison was available. Specificity was 85.2 percent.
"These results compare favorably with standard-of-care margin assessment," said Smith.
The trial met prespecified thresholds for removal of residual tumor and specificity but did not meet its prespecified sensitivity goal, which may be due to the trial's design, which did not include taking additional margin specimens when there were negative pFGS readings. Smith and colleagues are involved in ongoing studies that will obtain additional margin tissue to calculate sensitivity more precisely. They will also look in greater detail at how effectively pFGS clears margins, comparing outcomes to standard surgery and rates of recurrence.
"Overall, we found that pFGS removed tumor missed by standard lumpectomy and reduced the need for second surgeries for positive margins," said Smith. "Given its potential, pFGS merits evaluation in future trials and studies."
More information: Barbara L. Smith et al, Intraoperative Fluorescence Guidance for Breast Cancer Lumpectomy Surgery, NEJM Evidence (2023). DOI: 10.1056/EVIDoa2200333
Journal information: NEJM Evidence
Provided by Mass General Brigham






Post comments