
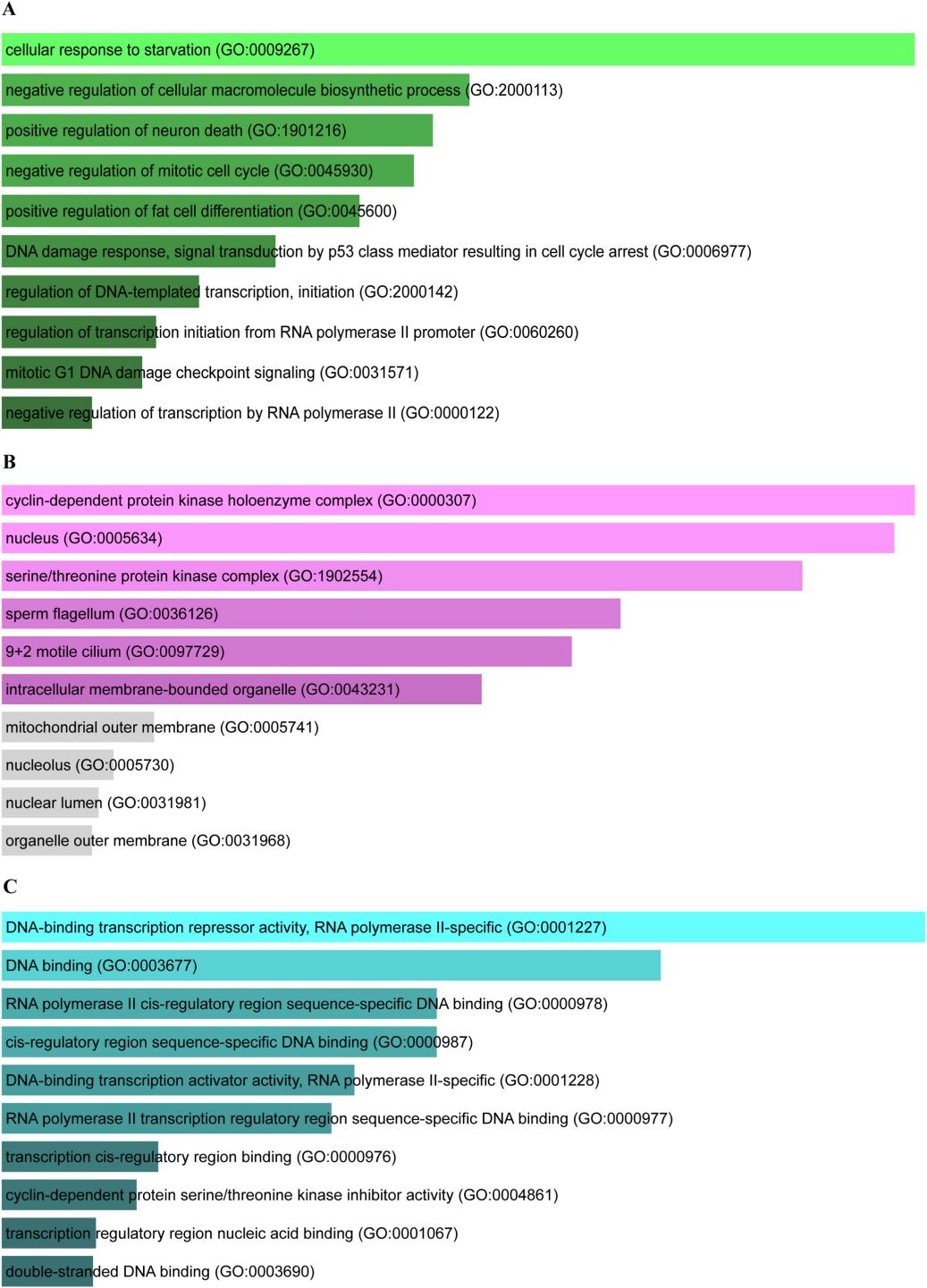
The top 10 GO terms of common genes between KOA and sarcopenia. (A) Biological Processes, (B) Cellular Component, (C) Molecular Function. GO, gene ontology; KOA, knee osteoarthritis.credit:DOI: 10.1016/j.afos.2023.08.005
Osteoarthritis of the knee is characterized by knee pain and dysfunction, and the main pathological features include cartilage loss, subchondral bone sclerosis, meniscus wear, and changes in the knee joint space. Reduced muscle strength and mass can induce KOA and aggravate its development [1]. Sarcopenia is a syndrome characterized by a slow decline in the strength and mass of skeletal muscles of the limbs. The prevalence of sarcopenia in 60-70 year olds ranges from 5% to 13% [2]. In patients with sarcopenia, the cross-sectional area of the quadriceps muscle is reduced by 12% to 19% compared with the normal population, and the muscle strength is reduced by 20% to 40% compared with the normal population. There indicated a strong association between KOA and sarcopenia [3].
Inflammatory factors are one of the risk factors for the development of sarcopenia. With the aging of the body, the body is in a chronic inflammatory state for a long time, and the levels of inflammatory factors such as interleukin (IL)-6 and tumor necrosis factor (TNF)-α increase in blood, causing muscle catabolism. Rom et al. [4] found that in the ubiquitinproteasome system (UPS), myostatin and muscle cyclin 1 regulate muscle protein catabolism. Inflammatory factors such as TNF-α can promote the expression of myostatin and muscle cyclin 1, which in turn promotes muscle catabolism and leads to muscle loss. Kauppinen et al. [5] found that IL-1 and TNF-α can also promote muscle catabolism through the nuclear factor-κB (NF-κB) signaling pathway. Inflammatory factors can trigger the onset or exacerbate the development of KOA. Increased levels of inflammatory factors in muscle can cause muscle stiffness, which in turn can lead to impaired joint mobility. Inflammatory factors such as IL-1 and TNF-α can activate transforming growth factor β-activated kinase 1, which induces the degradation of proteoglycans in the extracellular matrix, leading to the degradation of cartilage extracellular matrix, causing damage to articular cartilage and exacerbating the development of KOA. Ismail et al. found that some inflammatory factors can activate the NF-κB signaling pathway and promote muscle and articular cartilage decomposition [6].
Skeletal muscle is an important target organ for insulin. Under physiological conditions, insulin activates the AKT signaling pathway and inhibits the activity of UPS and Caspase-3 in vivo, thus maintaining the muscle mass. In addition, insulin inhibits protein hydrolysis through the p38 and mTOR/p70S6 pathways to maintain muscle mass. When insulin resistance occurs, caspase-3 and UPS are activated, promoting muscle catabolism and leading to sarcopenia [7]. Insulin resistance can induce KOA by accelerating synoviocyte and chondrocyte damage. Insulin can bind to the receptors on synovial cells, inhibit the inflammatory response in the knee joint, and play a protective role for synovial cells. When insulin resistance occurs, the inflammatory response in the knee joint cannot be suppressed, and the expression of TNF-α in the joint increases, further damaging the synovial cells. In addition, patients with insulin resistance often suffer from hyperinsulinemia, and increased insulin levels in the blood can lead to the destruction of articular cartilage, which in turn induces or aggravates KOA[8] . Increased insulin levels in the blood can lead to high activation of AKT and mTOR, resulting in a decrease in the number of autophagosomes . Autophagosomes have the function of removing intracellular damaged substances and stabilizing the intracellular microenvironment, and a decrease in the number of autophagosomes will seriously reduce the function of chondrocytes, which is closely related to the development of KOA [9].
Reference
Jones TL, Esa MS, Li KHC, Krishnan SRG, Elgallab GM, Pearce MS, Young DA, Birrell FN. Osteoporosis, fracture, osteoarthritis & sarcopenia: A systematic review of circulating microRNA association. Bone. 2021 Nov;152:116068.
Tong T, Quan H, Kim CK, Zeng W. Editorial: Role of nutrition in skeletal muscle atrophy and sarcopenia. Front Nutr. 2024 May 3;11:1395491.
Yang J, Jiang T, Xu G, Wang S, Liu W. Exploring molecular mechanisms underlying the pathophysiological association between knee osteoarthritis and sarcopenia. Osteoporos Sarcopenia. 2023 Sep;9(3):99-111.
Rom O, Reznick AZ. The role of E3 ubiquitin-ligases MuRF-1 and MAFbx in loss of skeletal muscle mass. Free Radic Biol Med. 2016 Sep;98:218-230.
Kauppinen A, Suuronen T, Ojala J, Kaarniranta K, Salminen A. Antagonistic crosstalk between NF-κB and SIRT1 in the regulation of inflammation and metabolic disorders. Cell Signal. 2013 Oct;25(10):1939-48.
Ismail HM, Didangelos A, Vincent TL, Saklatvala J. Rapid Activation of Transforming Growth Factor β-Activated Kinase 1 in Chondrocytes by Phosphorylation and K63 -Linked Polyubiquitination Upon Injury to Animal Articular Cartilage. Arthritis Rheumatol. 2017 Mar;69(3):565-575.
Hong SH, Choi KM. Sarcopenic Obesity, Insulin Resistance, and Their Implications in Cardiovascular and Metabolic Consequences. Int J Mol Sci. 2020 Jan 13;21(2):494.
Pérez-Baos S, Prieto-Potin I, Román-Blas JA, Sánchez-Pernaute O, Largo R, Herrero-Beaumont G. Mediators and Patterns of Muscle Loss in Chronic Systemic Inflammation. Front Physiol. 2018 Apr 24;9:409.
Saengsiwaritt W, Jittikoon J, Chaikledkaew U, Tawonsawatruk T, Honsawek S, Udomsinprasert W. Effect of vitamin D supplementation on circulating level of autophagosome protein LC3A, inflammation, and physical performance in knee osteoarthritis. Clin Transl Sci. 2023 Dec;16(12):2543-2556.






Post comments