
By Jonathan Cluett, MD
Medically reviewed by Scott Sundick, MD
Removal of the meniscus or meniscectomy is a surgical procedure in which the cartilage around your knee (called the meniscus), is completely or partially removed.
Your healthcare provider may suggest full or partial meniscus removal if you tear your meniscus. Meniscectomy can be done with local or general anesthesia (in which you are put to sleep) and it can decrease pain and restore mobility.
This article discusses what's involved in having the surgery, why it's done, how to prepare, and what to expect with surgery and recovery.
What Is a Meniscectomy?
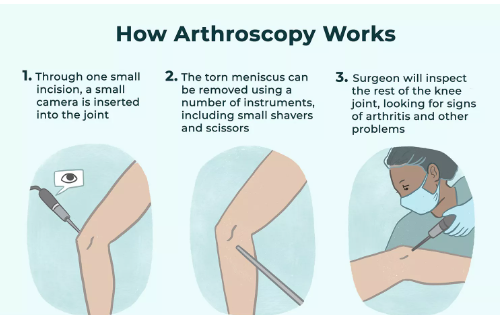
A meniscectomy is an outpatient, elective surgery to remove the torn meniscus in your knee. It’s typically done as an arthroscopic procedure. This involves small incisions, about a centimeter long, where an arthroscope (a small surgical camera) and small instruments are inserted so part or all of the meniscus can be removed.
Types of meniscectomy surgeries include:
Partial meniscectomy: Removes a small piece of the torn meniscus
Total meniscectomy: Removes the entire meniscus
In most cases, a partial meniscectomy is done to try to preserve as much of the cartilage as possible.1 Removal of an entire meniscus may increase the risk of arthritis about 10 years later.2 That’s because the meniscus helps decrease stress on the knee and provides shock absorption, stability, and joint lubrication. Without the meniscus, the impact of stress on the knee with activities is three times higher.3
Purpose of Meniscectomy
The meniscus is a tough, rubbery piece of cartilage that sits above the shinbone and provides cushioning and stability to the knee.
A meniscal tear can develop suddenly due to injury (such as when you twist your knee) or slowly due to a degenerative condition like osteoarthritis.1 As you age, the cartilage becomes less resilient. Because of this, injuries can happen more frequently, whether from playing sports or minor events such as stepping on an uneven surface.4
Damage to the meniscus can cause significant pain and mechanical symptoms such as popping or catching in the knee. A meniscectomy can help resolve these issues when more conservative treatment options are not effective.
The location of the tear may determine whether the meniscus can be repaired. The outer one-third of the meniscus has a rich blood supply. Tears in this “red zone” of the meniscus can often heal on their own or can be repaired through surgery.
If the tear in this area is small, it may be more likely to heal through non-surgical treatments, such as:5
The RICE protocol: Rest, ice (20 minutes at a time), compression (bandage), and elevation
Use of a brace
Activity modification
Non-steroidal anti-inflammatory medications
Steroid injections
Physical therapy6
The inner two-thirds of the meniscus, on the other hand, doesn’t have a rich blood supply. If a tear happens in this location, the meniscus may not have the ability to heal because of the lack of nutrients from the blood. A tear in this non-vascular part, or “white zone,” may require a meniscectomy.7
Magnetic resonance imaging (MRI) is used to confirm and assess the degree of a meniscal tear.
Contraindications
A meniscectomy is not recommended if at-home treatment can adequately reduce your symptoms or if your torn meniscus can be repaired via meniscus repair surgery. This can depend on the type and severity of the tear as well as its location.
Meniscal repair surgery tends to be more effective for people under 30 years of age who have the procedure within two months after the injury. Those over 30 may be less likely to have a successful surgical repair since meniscal tissue begins to weaken with age.4
Your healthcare provider will make a determination about your surgical options to suggest the best option for you based on your condition as well as your age, activity level, and general health. Some health conditions may increase the risk of complications.
Meniscus Surgery Risks
Potential risks and complications from a meniscectomy include:
Joint Stiffness
Stiffness of the knee joint can occur as a result of persistent swelling or scar tissue formation around the knee joint. For most people, the stiffness resolves with appropriate therapeutic intervention following surgery.8
Infection
Infection is an unusual complication of meniscus surgery, but it can occur. Infection can occur around the incisions, which is a superficial infection, or it can occur within the knee joint—a more serious, deeper infection.9
If the infection is around the incision, antibiotics will usually cure the infection. When the infection is deeper within the knee joint, additional surgical procedures to clean out the infection may become necessary. Having bacteria within the knee joint can cause significant damage to the cartilage of the joint, and therefore urgent treatment of any suspected infection is necessary.
Blood Clot
The risk of blood clots in the deep veins (deep vein thrombosis) of the lower leg is small, but it does occur. Blood clots can occur in anyone, but they are more common in people with specific risk factors for developing a clot.10
One risk factor for developing a blood clot is prolonged immobilization of the leg. So it's important to follow your healthcare provider's advice about moving your leg as much as possible to keep blood flowing and prevent blood clots.
Other risk factors include smoking, oral contraception, and blood clotting disorders, which may require additional precautions.
Arthritis
The long-term risk of arthritis in the knee after meniscus surgery is significantly higher compared to arthritis in the general population because some or all of the cartilage has been removed so there is less cushioning in the joint.
A 2018 study estimated the risk of osteoarthritis to be at least two times higher for people who had a partial meniscectomy.11
Symptoms from a degenerative tear will occasionally ease without surgery. Your healthcare provider may consider surgery if your knee is “locked,” persistently swollen, or keeping you from participating in normal activities for three to six months despite treatments such as physical therapy and injections.2
Before having surgery, you’ll have an appointment with your orthopedic surgeon. Your surgeon will do a physical exam to assess joint-line tenderness where the meniscus sits, pain when rotating the knee, clicking in the joint, and range of motion.6
You may need bloodwork or an electrocardiogram (ECG or EKG) to help plan your surgery and anesthesia.
How to Prepare for Meniscus Surgery
You’ll have an appointment to meet with the surgeon and ask any questions before the procedure. This will give you a chance to find out more about the risks and benefits specific to your condition.
Your surgeon will talk to you about the type of anesthesia you'll need, whether it’s general, regional, or local anesthesia. They’ll also let you know what to expect on the day of surgery and how you can prepare for the recovery phase.
Your healthcare provider may give you a prescription for pain medicine in advance of your procedure so you can have it filled and on-hand to use after surgery. You may be referred to a physical therapist before the surgery to get fitted for crutches and instructed on how to use them.4
Location
A meniscectomy is performed in a hospital operating room or outpatient surgical center. As part of your preparation, make arrangements for someone to bring you home after surgery.
What to Wear
You’ll be asked to change into a hospital gown before the procedure. Bring or wear loose shorts or pants that will be easy to fit over your bandage and dressing after surgery.
Food and Drink
Follow your surgeon’s instructions about when to stop eating and drinking before surgery. They may tell you to stop eating after midnight the night before the surgery because general anesthesia requires an empty stomach.12
Medications
Two weeks before your surgery, your healthcare provider may tell you to stop taking medications that can increase the risk of bleeding. These include aspirin, Advil (ibuprofen), Aleve (naproxen), and Coumadin (warfarin).12
To avoid complications, tell your healthcare provider about any prescriptions and over-the-counter medications you’re taking. This should include drugs, vitamins, supplements, and herbal remedies.
What to Bring
If you received crutches from your physical therapist, remember to bring them on the day of surgery. If you don’t have crutches, they should be given to you at the hospital after surgery.
Also bring any paperwork, your insurance card, and a form of identification like a driver’s license. Many hospitals will remind you to leave any valuable belongings (such as wallet, jewelry) at home.
Pre-Op Lifestyle Changes
If you currently smoke, let your surgeon know before the surgery. Smoking can increase your risk of complications because it affects blood flow, increasing the chance of a blood clot. The effects of smoking can also slow the healing of your bone and wounds.12
What to Expect on the Day of Surgery
Your pre-surgical nurse or physician’s assistant will meet with you to go over the details of your surgery with you. Your nurse will do a physical exam and check your vitals. You may be asked to sign consent forms before the surgery.
During the Surgery
Your surgery should last about one hour.4 Once you are in the operating room, the planned form of anesthesia will be administered:
If you have local anesthesia, your knee will be injected with medicine to numb the area. You may be given medications to relax you, but you’ll be awake throughout the procedure.
With regional anesthesia, pain medicine is injected into a space in your spine. You’ll be numb below the waist but awake during the surgery.12
With general anesthesia, you’ll receive medication to put you to sleep through an intravenous (IV) line in your arm or through a breathing mask. The anesthesiologist will monitor your vital signs throughout your procedure. When you’re asleep, your anesthesiologist may put a breathing tube in your windpipe to protect your airway.
Your surgeon then makes small holes, or portals, in your knee. An arthroscope, which includes a light and camera, is inserted into one of the incisions. One or more other incisions are used for the insertion of saline solution to help your surgeon see and to place the necessary surgical instruments that are used for your procedure.
Your surgeon will inspect the inside of your knee and look at your meniscus tear. Your surgeon will then cut and remove the torn piece with small instruments called punches. The edges of the meniscus are made smooth with a shaver, which is a motorized instrument with suction.
Saline is once again flushed through the knee to help rinse out any loose particles.6 Then the incisions are closed with stitches or surgical tape.2
After the Surgery
You’ll stay in the recovery room until your anesthesia wears off. While discharge requirements may vary, you’ll probably be able to go home when your medical team has determined that your vitals are stable and you’re able to urinate, drink fluids, and walk with your crutches.
You can usually go home the on same day of your surgery.4
Your knee will be wrapped with dressing and an elastic bandage, and you will be given an ice pack to help with pain and swelling. Leave the bandage in place per your surgeon's instructions.4
Recovery After Meniscus Surgery
Recovery time is usually four to eight weeks but can vary depending on the extent of your procedure, your age, and your overall health. You may want to arrange for someone to stay with you the first two days after the surgery to help you while you’re recovering. Most people can walk with crutches after the first couple of days.
One week after surgery: Some people are able to drive (as long as they’re not taking opiate pain medication). Some people can go back to work if their job doesn’t involve a lot of standing, walking, or heavy lifting.
Two weeks after surgery: You should have full range of motion in your knee.
Four to six weeks after surgery: You may be able to resume normal activity and walking for exercise if your strength and range of motion are restored. Check with your healthcare provider to find out when you can resume different activities and whether you need to make any modifications to protect your knee.
Your healthcare provider may suggest exercises to help you get back to normal faster. These exercises can help improve control of your leg muscles and knee range of motion. You may be able to do the exercises at home, or with the help of a physical therapist.6
You’ll likely need a follow-up appointment with your healthcare provider one to two weeks after the surgery.
Healing
You may have some pain and swelling for about a week after surgery. For the first two days after surgery, your surgeon may suggest putting ice on your knee for 20 minutes at a time several times a day to help reduce pain and swelling. You can help decrease swelling while resting by putting two or three pillows under your knee while laying flat on your back.4
Your surgeon will let you know when it’s safe to bathe or shower. They may advise covering your knee with plastic to keep your incisions dry and reduce the risk of infection.4
Use crutches to help keep stress off your knee while it’s healing. Your physical therapist will work with you to determine when you can stop using crutches. Usually, this can happen when you are able to comfortably put your full weight on your surgical leg.4
Pain medications, including opioids such as hydrocodone or oxycodone, may be prescribed for the first 48 hours, although they are typically not needed after this procedure.2 These medications can be safe if used properly and for a short amount of time. Follow your surgeon’s instructions to avoid misuse of opioids, which can lead to overdose, addiction, or death.
Your surgeon may recommend using over-the-counter pain medication thereafter. Most people are able to stop taking pain relief drugs after the first week.2
When to Call Your Surgeon or Healthcare Provider
The following are possible signs of complications and warrant medical evaluation:
Fever (101 degrees F or more)
Redness
Increasing pain that's not relieved by ice or medication
Drainage that’s pus-like or foul-smelling
Trouble breathing
Pain in your calf when you flex your foot
Swelling in your leg, ankle, or foot4
Possible Future Surgeries
People who have osteoarthritis and have a meniscectomy may be more likely to need knee replacement surgery down the road.
A 2016 study found that osteoarthritis patients who had an arthroscopic meniscectomy were three times more likely to need knee replacement surgery than osteoarthritis patients who didn’t have a meniscectomy.13
Talk to your healthcare provider if you have any questions about the effectiveness of meniscectomy for your condition and whether it might lead to future surgeries.
Sources
1.Cedars-Sinai Health Library. Medial and lateral meniscus tears.
2.University of Washington, Department of Orthopaedics and Sports Medicine. Meniscectomy.
3.Razi M, Mortazavi SMJ. Save the meniscus, A good strategy to preserve the knee. Arch Bone Jt Surg. 2020;8(1):1-4. doi:10.22038/abjs.2019.45438.2242
4.Cleveland Clinic. Meniscal tears.
5.NYU Langone Health. Nonsurgical treatments for meniscus tears.
6.American Academy of Orthopaedic Surgeons. Meniscus tears overview.
7.American Academy of Orthopaedic Surgeons. Meniscus tears.
8.Ghani H, Maffulli N, Khanduja V. Management of stiffness following total knee arthroplasty: A systematic review. The Knee. 2012;19(6):751-759. doi:10.1016/j.knee.2012.02.010
9.Balato G, Di donato SL, Ascione T, et al. Knee septic arthritis after arthroscopy: incidence, risk factors, functional outcome, and infection eradication rate. Joints. 2017;5(2):107-113. doi:10.1055/s-0037-1603901
10.Flevas DA, Megaloikonomos PD, Dimopoulos L, Mitsiokapa E, Koulouvaris P, Mavrogenis AF. Thromboembolism prophylaxis in orthopaedics: an update. EFORT Open Rev. 2018;3(4):136-148. doi:10.1302/2058-5241.3.170018
11.Persson F, Turkiewicz A, Bergkvist D, Neuman P, Englund M. The risk of symptomatic knee osteoarthritis after arthroscopic meniscus repair vs partial meniscectomy vs the general population. Osteoarthr Cartil. 2018;26(2):195-201. doi:10.1016/j.joca.2017.08.020
12.U.S. National Library of Medicine. Knee arthroscopy.
13.Rongen J, Rovers M, van Tienen T, Buma P, Hannink G. Increased risk for knee replacement surgery after arthroscopic surgery for degenerative meniscal tears: a multi-center longitudinal observational study using data from the osteoarthritis initiative. Osteoarthr Cartil. 2017;25(1):23-29. doi:10.1016/j.joca.2016.09.013
Additional Reading
Greis PE, Holmstrom MC, Bardana DD, Burks RT. Meniscal Injury: II. Management. J. Am. Acad. Ortho. Surg., May/June 2002; 10: 177-187. doi:10.5435/00124635-200205000-00004
By Jonathan Cluett, MD
Dr. Cluett is board-certified in orthopedic surgery. He served as assistant team physician to Chivas USA (Major League Soccer) and the U.S. national soccer teams.






Post comments