
By Colleen Doherty, MD
Published on July 26, 2023
Medically reviewed by Richard N. Fogoros, MD
A pulmonary embolism (PE) occurs when a blood clot (embolus) lodges within the main artery of the lungs. In most cases, the blood clot starts in one of the deep veins in the leg (deep vein thrombosis, or DVT) before traveling through the bloodstream to the lungs.1
Treating PE is critical to preventing complications like recurrent blood clots in the lung, right heart failure, cardiac shock, and even death. Despite being a medical emergency, most people recover well from a pulmonary embolus if diagnosed and managed promptly and effectively.
This article will explore the goals and steps taken to treat a pulmonary embolism. The wide range of PE treatment options and their indications will also be discussed.
Pulmonary Embolism
What Are the Goals of Pulmonary Embolism Treatment?
The goals of treating a pulmonary embolism are to:
Prevent the blood clot from becoming bigger
Prevent new blood clots from forming and subsequently traveling to the lung
Prevent serious complications
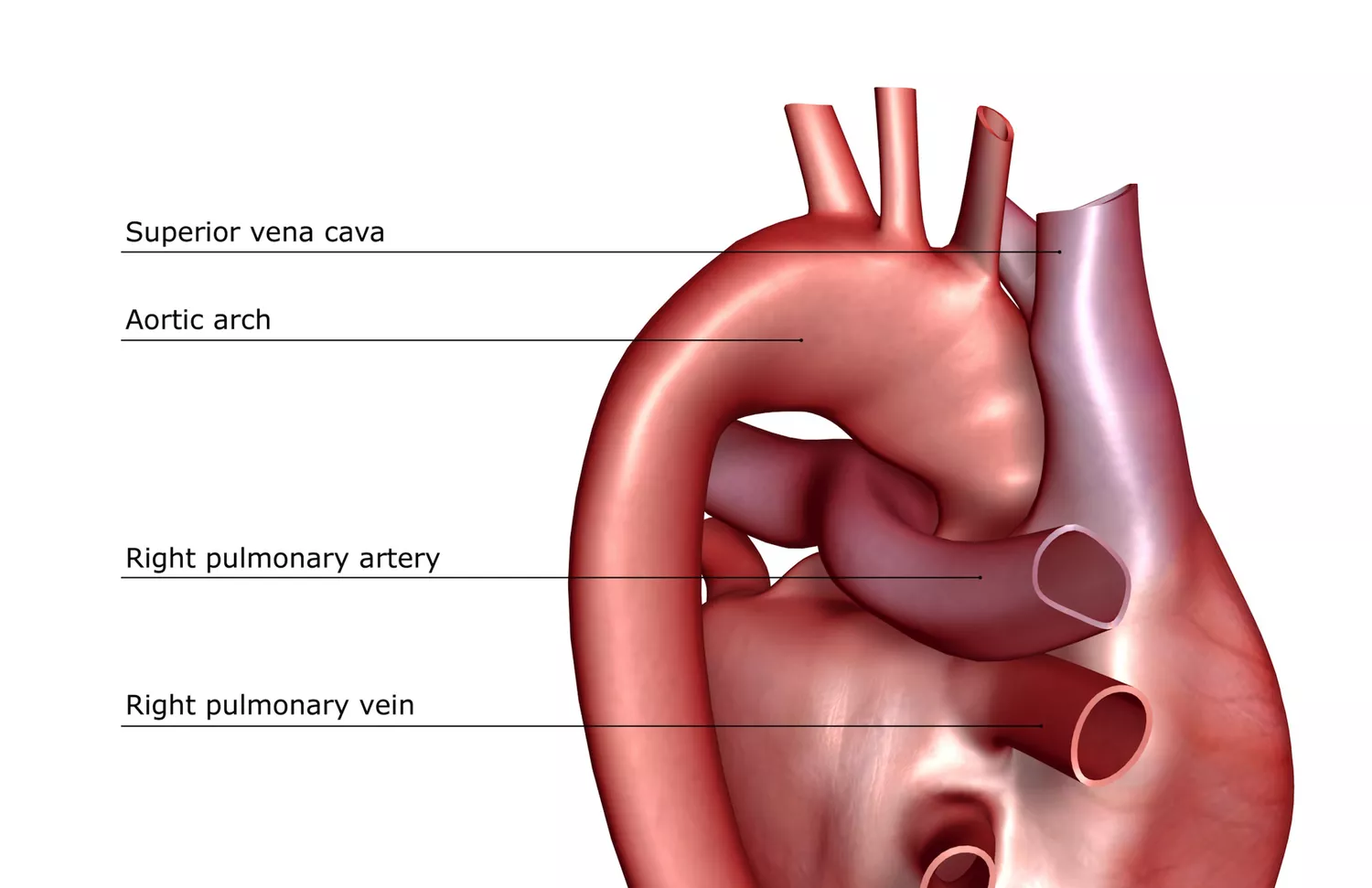
Right ventricular failure is a common complication of PE.2 The right ventricle is the lower right heart chamber. Blood is pumped from the right ventricle through the pulmonary artery into the lungs to be oxygenated.
If a blood clot blocks the pulmonary artery, the pressure within the artery rapidly increases. This pressure strains the right ventricle, potentially impairing its ability to pump enough blood into the lungs for oxygenation.
Right ventricular failure may result in low blood pressure (hypotension), abnormal heart rhythms (arrhythmias), and sometimes, cardiac shock and death.3
A late complication of PE is post-PE syndrome, an umbrella term for two diagnoses—chronic thromboembolic pulmonary hypertension (CTEPH) and chronic thromboembolic disease (CTED).4
Post-PE Syndrome: Seek Medical Attention
Contact a healthcare provider if you are experiencing persistent (for more than three months) trouble breathing (dyspnea) or exercise intolerance after being diagnosed with a pulmonary embolism.
How Does Pulmonary Embolism Treatment Work?
Treating a PE requires considering several factors, including a person's bleeding risk, symptoms, and functional status prior to the blood clot.
PE severity is classified into the following four categories determined by guidelines from the American Heart Association (AHA) and the European Society of Cardiology (ESC):5
Low-risk PE: A person is hemodynamically stable (no hypotension) with no evidence of right ventricle dysfunction or heart damage.
Intermediate-low-risk or submassive PE: A person is hemodynamically stable but has right ventricle dysfunction or an elevated blood troponin (a marker of heart damage).
Intermediate-high-risk or submassive PE: A person is hemodynamically stable but has right ventricle dysfunction and an elevated blood troponin.
High-risk or massive PE: A person is hemodynamically unstable, meaning they have a systolic blood pressure (the first number) of less than 90 millimeters of mercury (mmHg) or require vasopressor support (medications to increase blood pressure).
Massive PE Is Uncommon But Potentially Fatal
Among hospitalized people with PE, approximately 5% are high risk, and 40% to 60% are low risk. The average mortality (death) rate of high-risk individuals is around 30% within one month of having the PE, compared to 1% of low-risk individuals.5
How Long Before a Pulmonary Embolism Turns Fatal
What’s the Most Common Treatment?
The hallmark treatment for a pulmonary embolus is anticoagulation. Also known as blood thinners, anticoagulants prevent new blood clots from developing. They do not help break up or dissolve the clot, but their benefit in lowering the risk of death and PE recurrence is well proven.6
In most cases, anticoagulation is started as soon as a diagnosis of PE is suspected unless there is a clear contraindication (e.g., active or high risk of bleeding).
Pulmonary Embolism Diagnosis: The 3-Step Process
Anticoagulation is continued for three to 12 months, and sometimes indefinitely, depending on the clinical scenario and the person's bleeding risk.7
Anticoagulant agents include:
Heparin is given as an injection underneath the skin or intravenously (through the vein).
Low molecular weight heparin (LMWH)—for example, Lovenox (enoxaparin)—is given as an injection underneath the skin.
Arixtra (fondaparinux) is given as an injection underneath the skin.
Direct oral anticoagulant—for example, Xarelto (rivaroxaban) or Pradaxa (dabigatran) is taken as a pill.
Jantoven or Coumadin (warfarin) is a pill and requires monitoring with regular blood tests to ensure therapeutic levels.
Selecting an Anticoagulant
Choosing the right anticoagulant depends on multiple factors, including underlying medical problems (e.g., kidney disease), bleeding risk, and clinical judgment.
What If the Clot Is Large or Life-Threatening?
While anticoagulation remains a cornerstone in the treatment of PE, advanced and more invasive therapies that involve dissolving or removing the clot are considered in high-risk cases.
Dissolving the Clot
Thrombolytic therapy is considered for individuals with a massive PE, assuming the person is at low risk for any serious bleeding.8
With a massive PE, a person is hemodynamically unstable, meaning blood flow to their organs is restricted.9 Persistently low blood pressure is a key sign of hemodynamic instability.
In contrast to anticoagulants which only thin the blood, thrombolytics are drugs that work to actively and quickly dissolve or break up the clot. By breaking up the clot, blood flow through the pulmonary artery can be rapidly restored.
Thrombolytics include streptokinase, urokinase, and recombinant tissue‐type plasminogen activator. The drawback to using a thrombolytic is its potential to cause bleeding.8
Removing the Clot
If a person with a massive PE fails to respond to or has a contraindication to thrombolytic therapy, embolectomy is often considered.6
Embolectomy is a procedure in which the blood clot is removed using a catheter-directed technique or an operation that resembles traditional open heart surgery. Deciding between the two types of embolectomy depends on several factors, such as the expertise available within that hospital and the person's health status.
The catheter-directed embolectomy is a minimally invasive procedure usually performed under sedation by an interventional radiologist or surgeon.10
During this procedure, the provider does the following:
Makes a small cut in the patient's neck or groin area
Guides a catheter (a thin, flexible tube) into the affected pulmonary artery
Remove the clot using various techniques, like breaking up the clot into pieces and aspirating it out
A surgical embolectomy is performed under general anesthesia by a surgeon.11
During this operation, the surgeon does the following:
Makes a large cut through the breastbone in order to access the heart, lungs, and associated blood vessels
Places the person temporarily on a cardiopulmonary bypass machine which performs the work of the heart and lungs
Opens the affected pulmonary artery and removes the blood clot
What If Anticoagulation Doesn't Work?
If a person develops recurrent blood clots in the lung despite receiving anticoagulation, an inferior vena cava (IVC) filter may be placed.6
An inferior vena cava (IVC) filter is a small wire device that traps blood clots traveling from the legs to the lungs. Depending on the case, the filter may be placed temporarily or permanently.
IVC filters are placed in the inferior vena cava, a large vein in the abdomen that carries blood to the heart and lungs.
IVC Filter Placement
IVC filter placement is a minimally invasive procedure performed under sedation by an interventional radiologist. It involves threading a catheter through a small cut made in the groin. The catheter contains the collapsed filter, which expands and attaches to the walls of the inferior vena cava.
Besides blood clot recurrence despite therapeutic anticoagulation, IVC filter placement may be advised in the following scenarios:
The person has a contraindication to anticoagulation—perhaps they recently underwent surgery or have a history of a brain bleed.
It's anticipated that the person will eventually need to stop anticoagulation—perhaps they have metastatic cancer.
The person has significant heart or lung problems that make them vulnerable to potentially fatal complications if another PE occurs.
Managing Pulmonary Embolism
The duration of treatment for PE depends on numerous factors, including the type of treatment given and the person's bleeding risk. A hematologist (doctor specializing in blood disorders) can help guide management decisions.7
If you or a loved one is on an anticoagulant, take it as prescribed. Also, inform your healthcare provider before starting any new medication, vitamin, supplement, or over-the-counter drug.
Furthermore, it's common to bleed easily on an anticoagulant. You may notice minor gum bleeding, easy bruising, or heavier menstrual bleeding. Contact a provider if the bleeding is excessive or worsening.12
Also, seek medical attention if you fall or bump your head. Minor accidents and injuries can be serious for individuals on blood thinners.
Wear a medical identification bracelet or necklace noting the type of anticoagulant you are taking. This information is needed in case of a medical emergency.
Seek Emergency Medical Attention
Go to your nearest emergency room or call 911 if you experience the following symptoms:
Blood in your urine, stool, or vomit
Severe abdominal or back pain
Feeling light-headed or fainting
Trouble breathing, chest pain, or rapid heartbeat
Leg swelling, redness, tenderness, or warmth
Life Expectancy and Recovery After Pulmonary Embolism
Using Hypercoagulability Evaluations to Determine Cause
Sometimes a PE occurs because a person's blood has an unusually strong propensity to form clots—a condition called hypercoagulability.
After diagnosing you with PE, a healthcare provider will carefully evaluate your medical and family history to help determine whether the blood clot was triggered by an acquired risk factor or an inherited thrombophilia (a genetic condition that causes your blood to clot easily).13
Tarbox AK, Swaroop M. Pulmonary embolism. Int J Crit Illn Inj Sci. 2013;3(1):69-72. doi:10.4103/2229-5151.109427
Major risk factors for a blood clot are cancer and recent surgery, trauma, or immobilization. Moderate risk factors are hormone replacement therapy, smoking, pregnancy, and having obesity.
Causes and Risk Factors of Pulmonary Embolism
While not a complete list, types of inherited thrombophilia include:
Factor V Leiden
Protein C deficiency
Protein S deficiency
Antithrombin deficiency
Various blood tests are used to diagnose inherited thrombophilias.
Suppose you or a loved one is found to have an inherited thrombophilia. In that case, a hematologist may refer you to a genetic counselor to help decide if family members should be screened.
Summary
A pulmonary embolus (PE) is a potentially fatal blood clot in the main artery of the lungs. PE treatment aims to prevent complications and prevent the clot from enlarging and new clots forming.
The mainstay treatment for PE is taking an anticoagulant (a blood thinner). Sometimes, a small device called an IVC filter is placed in the body to prevent blood clots from traveling to the lungs from the legs. Advanced therapies that involve dissolving or removing the blood clot are less commonly performed.
Recovery from a PE depends on numerous variables, including the severity of the clot, bleeding risk, and the underlying cause.





Post comments