
by H. Lee Moffitt Cancer Center & Research Institute
Outcomes for patients with clear cell renal cell carcinoma have improved over the past decade due to the approval of immunotherapies, yet still there is a subset of patients who do not respond to this type of therapy.
Moffitt Cancer Center researchers have been working to better understand how the immune cell microenvironment contributes to patient outcomes in hopes of identifying biomarkers that predict responses to treatment. In a new article published in the Journal for ImmunoTherapy of Cancer, a team of Moffitt scientists reveals that the spatial organization of immune cells in the tumor microenvironment of clear cell renal cell carcinoma predicts patient outcomes.
Immunotherapies that activate immune cells against cancer cells have greatly changed the standard of care for many cancer types, including clear cell renal cell carcinoma. Several biomarkers, such as expression levels of the protein PD-L1 or the presence of CD8+ T cells, have been associated with improved outcomes to this type of therapy. However, these biomarkers have not had strong predictive value in clear cell renal cell carcinoma, suggesting that the immune tumor environment may be more unique and complex compared to other tumor types.
The tumor immune microenvironment is composed of many different types of immune cells. Some have antitumor activities, such as CD8+ T cells, while others have protumor activities, such as M2-like tumor associated macrophages. Patient outcomes to treatment are not solely dependent on the presence or absence of these cell types, and interactions among these different cells is likely important.
"We have seen previous studies show that tumor associated macrophages may interact with CD8+ T cells in clear cell renal cell carcinoma, and this interaction causes T cells to become exhausted and ineffective against tumor cells," said study author Brandon Manley, M.D., assistant member of the Genitourinary Oncology Department at Moffitt. "Our work provides a better understanding of the relationships and interactions between these different immune cells in the environment of clear cell renal cell carcinoma."
Manley and the team of researchers used an experimental approach that preserved the clear cell renal cell carcinoma tumor tissue and enabled them to determine precise spatial organization and distributions of immune cells in relation to tumor cells and the surrounding tumor environment called the stroma.
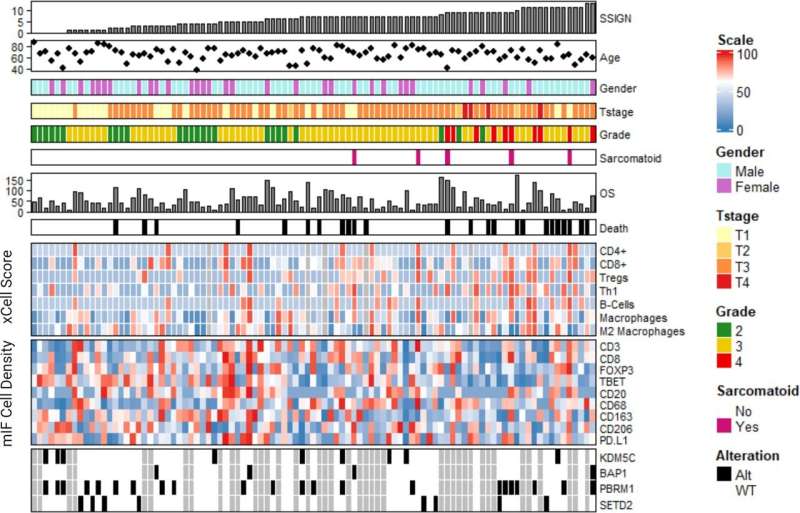
They analyzed tissue samples from 97 clear cell renal cell carcinoma patients and discovered that the highest density of immune cells is most often at the interface between the tumor and the surrounding stromal cells. Patients who had tumor associated macrophages that clustered into the stromal compartment had worse clinical stage and shorter survival than patients who had tumor associated macrophages that clustered more toward the tumor compartment.
The researchers used this information to develop a score based on the expression of 20 genes that could predict tumor associated macrophage clustering. They validated the score in different independent groups of patients and confirmed the association between gene expression, disease stage and survival.
The research team also analyzed the localization of tumor associated macrophages in relation to CD8+ T cells. They demonstrated that patients who had tumor associated macrophages colocalize with CD8+ T cells toward the stroma had poorer outcomes compared to patients who did not display colocalization or who had the cells colocalized toward the tumor area. They showed that these poor outcomes were associated with a high presence of CD8+ T cells that are in an exhausted, inactive state at the tumor-stroma interface.
"These findings demonstrate that specific cellular locations and spatial relationships contribute significantly to clinical and biological outcomes, highlighting that cellular phenotype and abundance may not adequately describe the clear cell renal cell carcinoma tumor microenvironment in the absence of geospatial context," Manley said.
More information: Nicholas H Chakiryan et al, Geospatial characterization of immune cell distributions and dynamics across the microenvironment in clear cell renal cell carcinoma, Journal for ImmunoTherapy of Cancer (2023). DOI: 10.1136/jitc-2022-006195
Provided by H. Lee Moffitt Cancer Center & Research Institute







Post comments