
by University of Texas M. D. Anderson Cancer Center
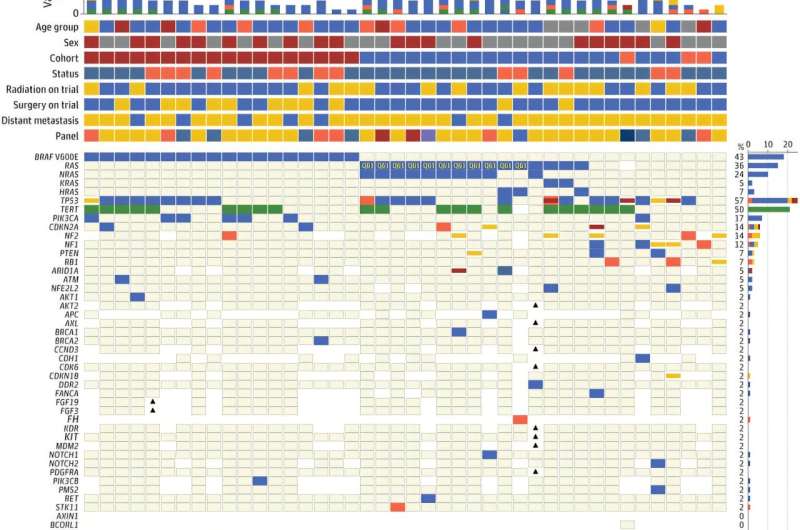
Oncoprint of targeted somatic gene variants of tumors in patients with anaplastic thyroid cancer (atc) enrolled in cohorts 1 to 3. Credit: JAMA Oncology (2024). DOI: 10.1001/jamaoncol.2024.4729
Researchers from The University of Texas MD Anderson Cancer Center have demonstrated that anti-PD-L1 immunotherapy in combination with mutation-directed targeted therapy extended overall survival (OS) in patients with anaplastic thyroid carcinoma (ATC).
Findings from the Phase II single center study appear in JAMA Oncology.
The trial enrolled 42 patients across three cohorts to evaluate mutation-matched targeted therapy and the immune checkpoint inhibitor atezolizumab. The median OS across all cohorts was 19 months, which compares favorably to the historical OS of five months for patients with ATC. The longest OS among the cohorts was 43.2 months in patients with BRAFV600E mutations—the longest OS published to date for systematic therapy in ATC.
"Patients with anaplastic thyroid carcinoma need treatments that work fast, and we saw promising results with this combination treatment approach. The takeaway from this study is that immunotherapy really does add benefit for patients," said principal investigator Maria Cabanillas, M.D., professor of Endocrine Neoplasia & Hormonal Disorders. "Based on these findings, we currently use this combination as our standard of care at MD Anderson for patients with ATC and BRAF mutations."
Anaplastic thyroid carcinoma is a rare and highly aggressive malignant tumor with a very poor prognosis. ATC often develops from differentiated thyroid cancer subtypes, such as papillary and follicular thyroid carcinoma, and each subtype has distinct driver mutations that can influence tumor behavior and progression.
Mutations in BRAF have therapeutic and prognostic implications and are seen in 40% of thyroid cancer patients. The trial enrolled 18 patients with BRAF-mutated ATC in cohort 1, who received treatment with atezolizumab plus the targeted therapy combination of vemurafenib and cobimetinib. The median OS was 43.2 months with an objective response rate (ORR) of 50%.
Cohort 2 enrolled 21 patients with RAS (NRAS, KRAS or HRAS) or NF1/2 mutations for treatment with cobimetinib plus atezolizumab. The combination achieved a median OS of 8.7 months and a 14% ORR.
Cohort 3 included three ATC patients with none of the above mutations who received bevacizumab plus atezolizumab. The median OS was 6.21 months and ORR was 33%.
This trial is also notable as it has been difficult historically to enroll patients with ATC in clinical trials, Cabanillas explained. This study had more permissive entry criteria that contributed to successful enrollment of 42 patients over four years. For example, the trial allowed patients to continue receiving chemotherapy during screening, given the potential for rapid disease progression. Additionally, the study allowed patients to administer the oral drugs through a feeding tube using alternative formulations.
The researchers observed side effects that were expected based on previous trials with these drugs. Among the most common adverse events for all cohorts were fatigue, lymphopenia, diarrhea and anemia. There were notable serious side effects in a few patients, including colonic and esophageal perforations.
"There are no approved and effective therapies for ATC with non-BRAF mutations, and we continue to focus our research in that area," Cabanillas said. "We are working to optimize outcomes for our patients. We want them to live longer and better lives, and this study offers hope for patients with ATC."
Limitations of this study include the absence of a controlled arm, which is a challenge in rare tumor trials, as well as the acceptance of radiation and surgery to remove the primary tumor, which may have contributed to the improvement in survival. However, the researchers argue that future ATC clinical trials should be designed to allow for surgery, as it may have contributed to the improved survival outcomes in this study.
More information: Maria E. Cabanillas et al, Anti–Programmed Death Ligand 1 Plus Targeted Therapy in Anaplastic Thyroid Carcinoma, JAMA Oncology (2024). DOI: 10.1001/jamaoncol.2024.4729
Journal information: JAMA Oncology
Provided by University of Texas M. D. Anderson Cancer Center





Post comments