
by University of Pittsburgh
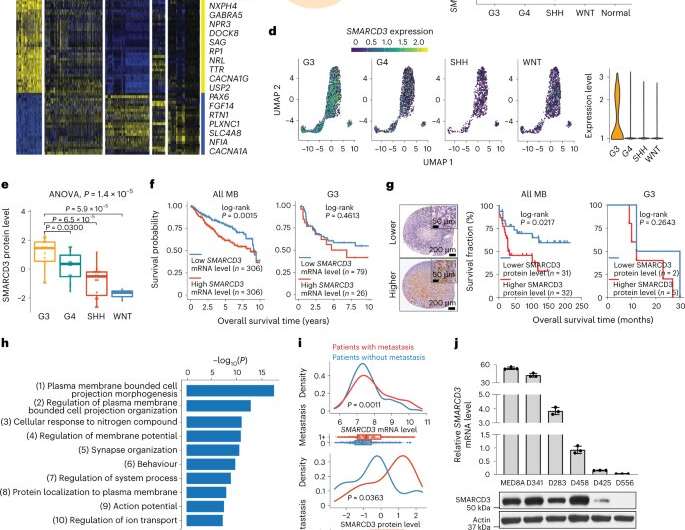
a, A heatmap of gene expression in the four MB subgroups (G3, group 4 (G4), SHH and WNT) and in unaffected (normal) tissues. Twofold change; false discovery rate (FDR) is less than 0.05. b, Venn diagram showing the overlapping SMARCD3 expression between G3-associated genes and epigenetic genes. c, Violin plot showing SMARCD3 mRNA expression using transcriptomics data from patients with MB. ANOVA, analysis of variance. d, Uniform manifold approximation and projection (UMAP) visualization (left) and violin plot (right) showing SMARCD3 mRNA expression based on scRNA-seq data from 25 patients with MB. e, Boxplot showing levels of SMARCD3 expression (nG3 = 14, nG4 = 13, nSHH = 15, nWNT = 3). f, Kaplan–Meier survival curve of patients comparing all MB subgroups (left) and G3 only (right) based on SMARCD3 mRNA expression level. g, Left, representative images of IHC staining for SMARCD3 levels in MB tissue microarrays. Right, log-rank test for survival fraction of patients comparing all MB subgroups and G3 only based on SMARCD3 level. h, Top ten biological pathways of the SMARCD3-associated genes in MB by GO analysis. i, Density plots (top) and boxplots (bottom) showing the association between metastasis status (0, no metastasis; 1+, metastasis at diagnosis) and SMARCD3 mRNA (n0 = 397, n1+ = 176) and protein (n0 = 23, n1+ = 20) expression levels in primary MB samples. j, RT–qPCR (top) and immunoblotting (bottom) analyses showing SMARCD3 mRNA (n = 3) and protein levels in six G3 MB cell lines. k, Representative haematoxylin and eosin (H&E) images showing primary tumors (yellow dashed lines) and brain and spinal metastatic tumors (red dashed lines) in six orthotopic xenograft models derived from G3 MB cell lines. Images are representative of three independent mice, with similar results obtained (k). Each dot represents one bulk sample (c,e,i) or one cell (d). n represents the number of human patients (a,c,e,f,g,i) or biologically independent samples (j). Data are presented as the mean ± s.d. P values were calculated using two-tailed Welch’s t-test with FDR correction (c,e,i) or two-tailed accumulative hypergeometric distribution (h). Credit: Nature Cell Biology (2023). DOI: 10.1038/s41556-023-01093-0
New research pinpoints a key cause of metastasis from an aggressive form of brain cancer in children and provides a potential new therapy for treating these tumors in the future.
In a paper published in Nature Cell Biology, physician-scientists from the University of Pittsburgh and UPMC Children's Hospital of Pittsburgh discovered that medulloblastomas hijack a skill that normal brain cells use during their early development and then manipulate it to help tumors spread.
"Children with medulloblastomas that have not yet metastasized may have a high likelihood of long-term survival, but if those tumors have spread, the survival rate is significantly reduced," said senior author Baoli Hu, Ph.D., assistant professor of neurological surgery at Pitt. "Longstanding challenges that we face in the field include understanding how tumors are able to spread and how we can stop tumor metastasis."
Brain tumors are the leading cause of cancer death in children. The most common malignant children's brain tumor is medulloblastoma, which form in a region of the brain called the cerebellum, with about 500 new cases diagnosed in the U.S. each year. Medulloblastomas are commonly treated with surgery followed by radiation and chemotherapy, but in up to one-third of children, the tumor will metastasize, or spread out to tissues and organs beyond where the tumor originated. When tumor cells spread, treatments no longer work and the outcomes are grim.
To learn how medulloblastoma cells metastasize, Hu and his team leveraged patient and experimental mouse data. They found that levels of a gene called SMARCD3 were significantly higher in metastatic tumors compared to those that had not spread.
They also showed that SMARCD3 hijacks neurodevelopmental signaling pathways to promote tumor cell spreading. These pathways are used by healthy brain cells during early cerebellar development and are shut off when the cerebellum matures.
Next, the researchers targeted these pathways with a drug called dasatinib, which has been approved to treat leukemia in the clinic. In a mouse model of medullobastoma, dasatinib preferentially killed metastatic tumors with higher levels of SMARCD3, suggesting that the drug causes little or no harm to normal brain cells and could be safe for treating patients with medulloblastoma metastasis.
"We've been thinking of medulloblastoma metastasis from the perspective of neuroscience and understanding how abnormal brain development causes and influences brain tumors," said Hu. "This approach helped us to pinpoint fundamental mechanisms of medulloblastoma metastasis, which will help us develop safe, effective and personalized treatments for children with this devastating brain cancer."
More information: Han Zou et al, A neurodevelopmental epigenetic programme mediated by SMARCD3–DAB1–Reelin signalling is hijacked to promote medulloblastoma metastasis, Nature Cell Biology (2023). DOI: 10.1038/s41556-023-01093-0
Journal information: Nature Cell Biology
Provided by University of Pittsburgh





Post comments