
by SPIE
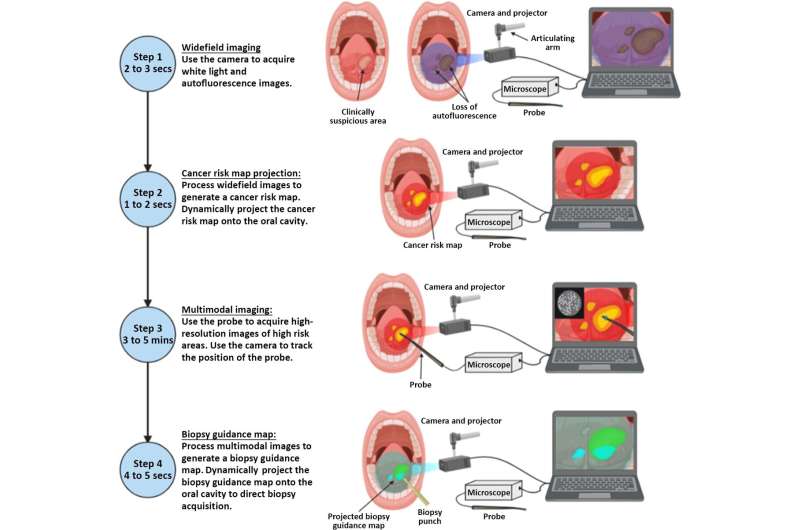
Imaging workflow of the ABGS. Step 1: widefield images are acquired using the camera and projector. Step 2: a cancer risk map is generated and projected onto the oral cavity. Step 3: multimodal images are acquired from the highlighted high-risk regions of tissue. Step 4: the multimodal image data are processed to generate and physically project a biopsy guidance map onto the oral cavity. Credit: Journal of Biomedical Optics (2023). DOI: 10.1117/1.JBO.28.1.016002
Oral cancer is a globally prevalent disease with an astonishingly low five-year survival rate of less than 50%. A key factor for its poor prognosis is delayed diagnosis resulting in more late-stage oral cancers. At these later stages, treatment becomes less effective and harsher on the body. Hence, many scientists aim to develop and improve diagnostic techniques for the early detection of oral cancer.
At present, the gold standard for the diagnosis of most oral cancers is biopsy of suspicious oral lesions and pathologic analysis of the extracted small amounts of tissue. However, it is extremely important that clinicians biopsy the areas within the abnormal lesion with the worst disease. Currently, the decision whether or not to perform a biopsy, and the optimal biopsy site, are based on clinical examination, which greatly depends upon the experience of the examining clinician.
To help identify high-risk regions, clinicians can also use commercially available imaging techniques based on autofluorescence to detect abnormal tissue at the macroscopic level, although current autofluorescence technologies suffer from low specificity for neoplastic disease.
Researchers have developed mechanisms to combine multiple imaging modalities to better identify optimal biopsy locations with greater accuracy than currently available techniques. Although these multimodal imaging techniques and supporting software tools have progressed considerably in recent years, clinicians still must observe the results on a computer screen and draw conclusions on where to perform biopsies by mentally translating the target locations from the screen to the patient's mouth.
This translation process presents a level of difficulty in precisely identifying the best biopsy location. What if the imaging system could not only pinpoint the best locations to biopsy within the patient's mouth in real time, but also project these optimal biopsy locations onto the oral mucosa?
In a recent study published in Journal of Biomedical Optics (JBO), a team of researchers co-directed by Rebecca Richards-Kortum from Rice University (Houston, USA) and Ann Gillenwater from The University of Texas M. D. Anderson Cancer Center (Houston, USA), presented a low-cost, portable imaging platform as a solution to this problem—the active biopsy guidance system (ABGS).
"ABGS is a multimodal imaging-based tool with a projection system, supported by a complete software architecture, which integrates widefield imaging, microscopic imaging, and real-time projection of cancer risk maps. This tool can help clinicians perform oral biopsies with greater precision," says Jackson Coole, lead author of the study, while describing the proposed solution.
Using the ABGS involves four key steps. First, the clinician uses a widefield camera to take pictures of the patient's oral cavity. Next, these captured white light and autofluorescence images are processed on a laptop, which uses analysis software to generate a cancer risk map.
Next, the cancer risk map is transmitted to a digital light projector, which physically projects the map to highlight the most suspicious-looking tissue zones in the oral cavity. These two steps can be completed in a matter of seconds to get the cancer risk map projected onto the oral cavity as soon as possible.
The third step involves using a flexible probe connected to a microscope to acquire high-resolution microscopy images of the high-risk areas highlighted by the projector. With the support of a tracking algorithm, the system can determine the probe's position and associate the microscopy images to the corresponding macroscopic location within the oral cavity. This imaging step is typically completed in less than five minutes.
Finally, the system analyzes the multimodal images obtained and computes a biopsy guidance map based on the results. Similar to the cancer risk map, the biopsy guidance map is projected onto the oral cavity of the patient in real time to highlight the tissue regions where the clinician should consider taking biopsies.
"We tested the ABGS at the University of Texas M. D. Anderson Cancer Center on multiple patients with oral lesions. It showed promising results in guiding clinicians to the most critical parts of suspicious lesions," adds Richards-Kortum. Impressed by the proposed system, JBO Editor-in-Chief Brian Pogue remarks, "This is a solid technical development in the difficult field of surgical guidance, where optical sampling can really make a difference."
Notably, the imaging modalities, probing tools, and detection algorithms used in the ABGS can also be modified based on different types of cancer.
More information: Jackson B. Coole et al, Multimodal optical imaging with real-time projection of cancer risk and biopsy guidance maps for early oral cancer diagnosis and treatment, Journal of Biomedical Optics (2023). DOI: 10.1117/1.JBO.28.1.016002
Journal information: Journal of Biomedical Optics
Provided by SPIE





Post comments