
by Carla K. Johnson

Jill Feldman, 54, poses for a photo at her home in Deerfield, Ill., Friday, Jan. 19, 2024. Lung cancer patient and advocate Jill Feldman takes pills at home that shrink tumors by blocking a signal that tells cancer cells to grow. Credit: AP Photo/Nam Y. Huh
For cancer patients, the harsh side effects of powerful drugs have long been the trade-off for living longer. Now, patients and doctors are questioning whether all that suffering is necessary.
They've ignited a movement to radically change how new cancer drugs are tested, with the U.S. Food and Drug Administration urging drugmakers to do a better job at finding the lowest effective dose, even if it takes more time.
Advances in treatment mean millions of people are surviving for years with incurable cancers. Jill Feldman, 54, of Deerfield, Illinois, has lived 15 years with lung cancer, thanks to that progress. Her parents both died of lung cancer months after their diagnoses.
But her cancer drug causes joint pain, fatigue and mouth sores that make eating and drinking painful.
"If you drink something that's too hot, you really burn your mouth. That's how my mouth feels 24/7," Feldman said.
She has lowered the dose with her doctor's blessing but she wants drugmakers to study lower doses early in the research process.
"No one should have to endure avoidable harmful effects of treatment," she said.
Unlike in other diseases, cancer drug development has focused on finding what's called the "maximum tolerated dose."
Photos and a sign are seen at Jill Feldman's home in Deerfield, Ill., Friday, Jan. 19, 2024. Lung cancer patient and advocate Jill Feldman takes pills at home that shrink tumors by blocking a signal that tells cancer cells to grow. Credit: AP Photo/Nam Y. Huh
To speed testing of chemotherapy drugs, researchers ramp up the dosage in a few people in early studies to determine the highest possible dose patients can tolerate. That "more is better" philosophy works for chemotherapy, but not necessarily for newer cancer drugs—like the one Feldman takes—which are more targeted and work differently.
Chemotherapy is like a battering ram where aggressive strikes are a good strategy. But newer cancer drugs are more like having a front door key. They target a mutation that drives cancer cell growth, for example, or rev up the body's immune system to join the fight.
"You might only need a low dose to turn off that cancer driver," said Dr. Lillian Siu, who leads cancer drug development at the Princess Margaret Cancer Center in Toronto. "If you can get the same bang for your buck, why go higher?"
Through a program called Project Optimus, the FDA is pushing drugmakers to include more patients in early dose-finding trials to get better data on when lower doses can work. A key motivation for the project was "the growing calls from patients and advocates that cancer drugs be more tolerable," said FDA spokesperson Chanapa Tantibanchachai in an email.
Many of the new cancers drugs were developed using the old strategy. That leads to problems when patients skip doses or stop taking the drugs because of side effects. Some dose recommendations have been officially lowered after the drugs were approved. Other dose-lowering happens one patient at a time. Nearly half of patients in late-stage trials of 28 targeted therapy drugs needed to have their doses lowered, according to one study.
"We were pushing the dose as high as we could go," said Dr. Patricia LoRusso, who leads drug discovery at Yale Cancer Center. "You get side effects and then you have to stop the drug to recover from the side effects and the tumor can grow."
There's also huge patient-to-patient variation. The amount of a pill that reaches the bloodstream can vary because of liver and kidney function and other differences. But that means lowering the dose for everyone risks underdosing some patients, LoRusso said.
A prescription bottle named osimertinib (brand name: Tagrisso) is seen on a table at Jill Feldman's home in Deerfield, Ill., Friday, Jan. 19, 2024. Lung cancer patient and advocate Jill Feldman takes pills at home that shrink tumors by blocking a signal that tells cancer cells to grow. Credit: AP Photo/Nam Y. Huh
"The challenge is: Where is the sweet spot?" LoRusso said.
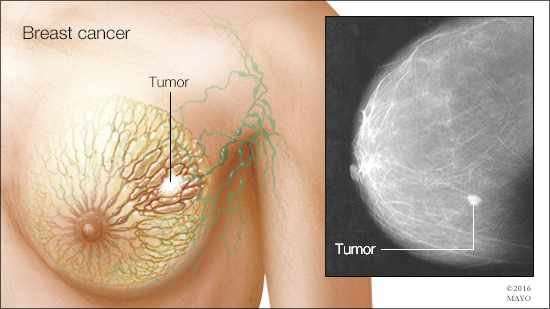
Dr. Julie Gralow, chief medical officer of the American Society of Clinical Oncology, is planning a 500-patient study to test lower doses of two drugs for breast cancer that has spread.
The study will compare two strategies: Starting treatment at the full dose then lowering the dose for side effects versus starting with a lower dose and increasing dosage if the patient does well.
Much of the questioning of high doses has come from metastatic breast cancer patients, including the Patient Centered Dosing Initiative, which has done influential surveys of patients and cancer doctors.
"We will be on treatment for the rest of our lives," said Lesley Kailani Glenn, 58, of Central Point, Oregon. "We want to try to live the best that we can, knowing that treatment is never-ever going to stop."
During the 11 years she's lived with the disease, she has summited Mount Whitney in California, hiked the Cinque Terra in Italy and started a nonprofit.
When Glenn learned how cancer drug research favors high doses, she started working with her doctor. She has taken drugs at lower doses and even lower when she can't live with the side effects. Diarrhea is her deal-breaker: She wants to be able to walk her dog or shop for groceries without worrying about a bathroom emergency.

A prescription bottle named osimertinib (brand name: Tagrisso) is seen on a table as Jill Feldman looks at her prescription bottle at her home in Deerfield, Ill., Friday, Jan. 19, 2024. Lung cancer patient and advocate Jill Feldman takes pills at home that shrink tumors by blocking a signal that tells cancer cells to grow. Credit: AP Photo/Nam Y. Huh
"The last thing we want to do is have our quality of life stolen from us," Glenn said.
Through Project Optimus, the FDA is encouraging drug developers to conduct more head-to-head dosing comparisons. That could slow down the process, said Dr. Alice Shaw, who leads early cancer drug development at Novartis.
"That will require more patients and then, as you can imagine, also will require more time to identify, enroll and treat those patients," said Shaw said. Adding six months to a year to the process, Shaw said, needs to be balanced against the urgent need for new cancer drugs.
But getting the dose right early will in the long run lead to more effective drugs, said Dr. Timothy Yap, a drug developer at MD Anderson Cancer Center in Houston. "If the patients are not taking the drug, then it's not going to work."
© 2024 The Associated Press. All rights reserved. This material may not be published, broadcast, rewritten or redistributed without permission.






Post comments