
by Ludwig Institute for Cancer Research
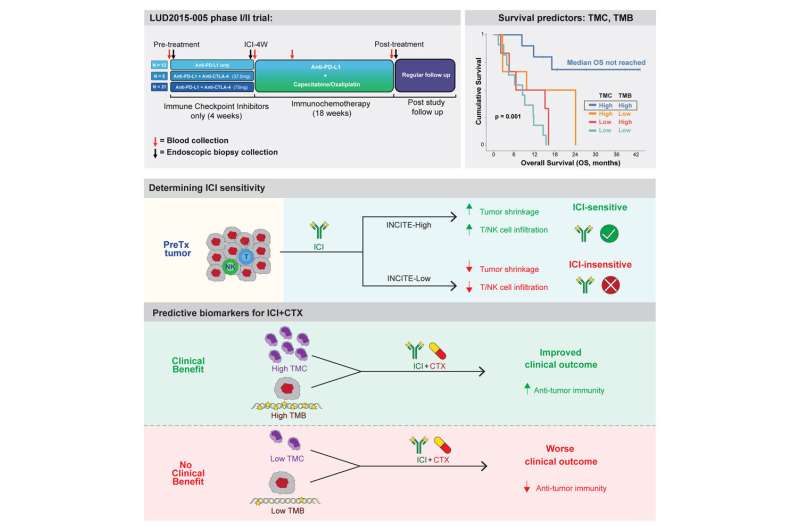
Graphical Abstract. Credit: Cancer Cell (2023). DOI: 10.1016/j.ccell.2023.06.006
A Ludwig Cancer Research study has discovered that the presence of relatively high numbers of immune cells known as monocytes in tumors is linked to better outcomes in esophageal cancer patients treated with a combination of chemotherapy and immunotherapy, or immunochemotherapy.
Esophageal cancer is the sixth leading cause of cancer mortality worldwide, and the incidence of esophageal adenocarcinoma has been climbing at a relatively swift clip over the past 40 years. Survival times for inoperable or metastatic forms of the cancer range from 6 to 12 months.
Led by Ludwig Oxford Director Xin Lu and former graduate student Thomas Carroll and published in the current issue of the journal Cancer Cell, the study also shows that the degree to which a tumor's malignant cells are mutated is similarly predictive of survival outcomes. Further, combining measurement of tumor mutational burden (TMB) and tumor monocyte content (TMC) better predicts treatment response than either measurement alone.
This suggests that the combined measurement is a potential biomarker for the selection of patients likely to benefit from immunochemotherapy.
"Some cancer patients respond to treatment while some do not, and still others respond only partially," said Lu. "The challenge is to understand why certain people fall into each category and identify the molecular bases of their heterogeneous responses."
A clinical trial (LUD2015-005) launched in 2015 by Ludwig Oxford offered a unique opportunity to address this challenge. The 35 patients with inoperable esophageal adenocarcinoma enrolled in this trial, unlike those in many others, received four weeks of immunotherapy with immune checkpoint inhibitors (ICI) alone (either anti-PD-L1, or anti-PD-L1 and anti-CTLA-4) before undergoing 18 weeks of combination immunochemotherapy.
Both healthy and cancerous biopsies were collected from the patients at multiple time points and from multiple sites over the course of their treatment. The researchers then performed single cell RNA sequencing (scRNA-seq) on 65,000 cells from a subset of the clinical trial patients to generate a detailed cellular atlas of the upper gastrointestinal tract, which served as a reference map of all the cell types that can be found in esophageal cancers.
Due to technical and other challenges associated with scRNA-seq—which analyzes the RNA output of individual cells—such analysis was only performed on 8 of the 35 EAC patients in the clinical trial. However, the biopsies of all patients underwent bulk RNA sequencing, a much more cost-effective alternative.
The team then used computational methods—deconvolution algorithms—to determine with high confidence the proportion of different cell types in each biopsy. Deconvolution is a computational tool that combines the biological insights from scRNA and bulk RNA sequencing while compensating for the particular weaknesses of each method—high cost and low resolution, respectively.
"In clinical research, we have to find ways to get as much information as possible from each precious sample. In this case, we wanted to use single-cell sequencing on a subset of those samples to gain detailed insight into the cell composition of these tumors, and combine that knowledge with the statistical power of conducting bulk RNA sequencing on everyone. That's what deconvolution attempts to do," explained Carroll.
Deconvolution revealed that the number of monocytes in the tumor before treatment was the most reliable predictor of outcome. This finding was surprising because ICI primarily targets the immune system's T cells, which lead the assault on tumors. "We found that pre-treatment T cell markers are not at all useful in predicting long-term patient outcomes for the treatment used in this trial," Carroll said.
The researchers hypothesize that the patients with high TMC can generate more pro-inflammatory immune cells from the monocytes in response to ICI therapy than patients with low TMC. Supporting this, they found that after four weeks of ICI, TMC-high patients showed a higher level of dendritic cells and M1 macrophages, which elicit pro-inflammatory or "tumor-killing" responses, while TMC-low patients had more anti-inflammatory or "tumor-supporting" M2 macrophages.
"We don't have the formal demonstration of this yet, and that's where the future research will be," Lu said.
Using publicly available data, the team also confirmed that the link between high TMC and improved outcomes held for the most common forms of gastric cancer as well.
Aside from identifying the combination of TMB and TMC as potential biomarkers for response to immunochemotherapy, the researchers report that expression of PD-L1—a protein targeted by ICI in the clinical trial—is not a good predictor of patient outcomes for such therapies. They also identify a novel T cell inflammation signature (INCITE) that correlates with ICI-induced tumor shrinkage. This signature could serve as a general indicator of a patient's responsiveness to immunotherapy, irrespective of their cancer.
More information: Thomas M. Carroll et al, Tumor monocyte content predicts immunochemotherapy outcomes in esophageal adenocarcinoma, Cancer Cell (2023). DOI: 10.1016/j.ccell.2023.06.006
Journal information: Cancer Cell
Provided by Ludwig Institute for Cancer Research





Post comments